Pharmacotherapeutic group: Hepatitis A vaccines.
ATC Code: J07BC02.
Pharmacology: Pharmacodynamics: Havrix confers immunisation against HAV by stimulating specific immune responses evidenced by the induction of antibodies against HAV.
Immune response: In clinical studies, 99% of vaccinees seroconverted 30 days after the first dose. In a subset of clinical studies where the kinetics of the immune response -were studied, early and rapid seroconversion was demonstrated following administration of a single dose of Havrix in 79% of vaccinees at day 13, 86.3% at day 15, 95.2% at day 17 and 100% at day 19, which is shorter than the average incubation period of hepatitis A (4 weeks) (see Pharmacology: Toxicology: Preclinical Safety data).
Persistence of the immune response: In order to ensure long term protection, a booster dose should be given between 6 and 12 months after the primary dose of Havrix 1440 Adult or Havrix 720 Junior. In clinical trials, virtually, all vaccinees were seropositive one month after the booster dose.
However, if the booster dose has not been given between 6 and 12 months after the primary dose, the administration of this booster dose can be delayed up to 5 years. In a comparative trial, a booster dose given up to 5 years after the primary dose has been shown to induce similar antibody levels as a booster dose given between 6 and 12 months after the primary dose.
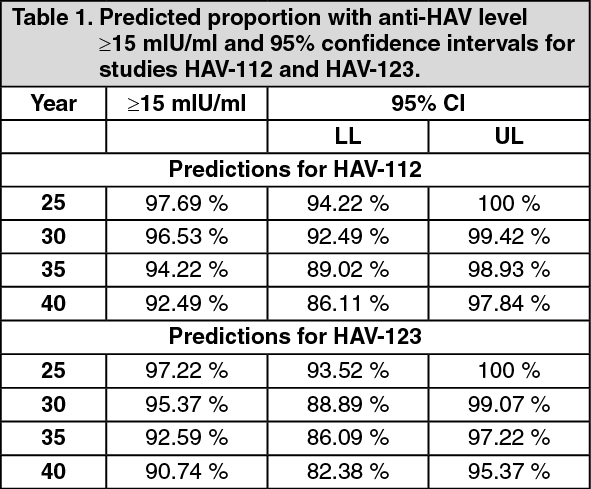
Long term persistence of hepatitis A antibody titres following 2 doses of Havrix given 6 to 12 months apart has been evaluated. Data available after 17 years allows prediction that at least 95% and 90% of subjects will remain seropositive (≥15 mIU/ml) 30 and 40 years after vaccination, respectively. (See Table 1).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Current data do not support the need for booster vaccination among immunocompetent subjects after a 2 dose vaccination course.
Efficacy of Havrix for outbreak control: The efficacy of Havrix was evaluated in different community-wide outbreaks (Alaska, Slovakia, USA, UK, Israel and Italy). These studies demonstrated that vaccination with Havrix led to termination of the outbreaks. A vaccine coverage of 80% led to termination of the outbreaks within 4 to 8 weeks.
Impact of mass vaccination on disease incidence: A reduction in the incidence of hepatitis A was observed in countries where a two-dose Havrix immunisation programme was implemented for children in their second year of life: In Israel, two retrospective database studies showed 88% and 95% reduction in hepatitis A incidence in the general population 5 and 8 years after the implementation of the vaccination program, respectively. Data from National Surveillance also showed a 95% reduction in hepatitis A incidence as compared to the pre-vaccination era.
In Panama, a retrospective database study showed a 90% reduction in reported hepatitis A incidence in the vaccinated population, and 87% in the general population, 3 years after implementation of the vaccination programme. In paediatric hospitals in Panama City, confirmed acute hepatitis A cases were no longer diagnosed 4 years after implementation of the vaccination programme.
The observed reductions in hepatitis A incidence in the general population (vaccinated and non-vaccinated) in both countries demonstrate herd immunity.
Toxicology: Pre-clinical Safety Data: Appropriate safety tests have been performed.
In an experiment in 8 non-human primates, the animals were exposed to an heterologous hepatitis A strain and vaccinated 2 days after exposure. This post exposure vaccination resulted in protection of all animals.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
